
An anterior cruciate ligament (ACL) injury is a potentially devastating occurrence for any individual or athlete. The physical, mental, and financial burden can be enormous. According to a paper from the Journal of Athletic Training in 2013, “anterior cruciate ligament injuries often require surgical repair followed by extensive long-term rehabilitation. An estimated $1 billion is spent annually for ACL reconstructions in the United States” (1).
When following the proper time allocation for ACL knee injury therapy, rehabilitation times can range anywhere from six months to two years. Depending on the athlete’s level of competition and time of year, the pressure and stress on an athlete to return to sport prematurely can be great. Additionally, news reports of professional athletes (i.e. Adrian Peterson) returning to the highest level of competition in extremely short periods of time place additional mental stress on individuals to return to sport far too early.
Athletes aren’t the only ones returning to physical activity before they should. Often, non-athletes with an ACL injury return to weekend activities such as skiing, basketball, soccer, or jogging before they are truly ready, placing themselves at risk for graft failure. Re-tear rates range anywhere from six to 27 percent, with a risk of re-injury being in both the surgical and non-surgical knee (2).
In 2016, a study in the British Journal of Sports Medicine concluded that those who do not meet six clinical discharge criteria before returning to a sport are four times more likely to have a graft rupture (3). The six criteria are:
| Return-to-sport tests | Discharge permitted when the following met: |
| 1. Isokinetic test at 60, 180, and 300°/s | Quadriceps deficit < 10% at 60°/s |
| 2. Single hop | Limb symmetry index > 90% |
| 3. Triple hop | Limb symmetry index > 90% |
| 4. Triple crossover hop | Limb symmetry index > 90% |
| 5. On-field, sports-specific training | Fully completed |
| 6. T-test of agility | < 11 s |
Tests Explained:
- Isokinetic testing usually involves a Biodex machine that gives objective data on hamstring and quadriceps strength at different speeds. In the study, the authors chose the speeds 60, 180, and 300°/s.
- Single hop for distance simply compares the distance on a single maximum jump starting on one leg and landing on the same leg. (see figure A below)
- Triple hop takes the distance on three consecutive jumps starting and finishing on the same leg. (see figure B below)
- Triple crossover jump takes the distance of three consecutive jumps crossing over a line each time, landing on the same leg to finish. (see figure C below)

- On-field, sport-specific training requires movements and plyometrics that mimic the requirements in the sport or activity of the athlete or individual.
- Agility T-test
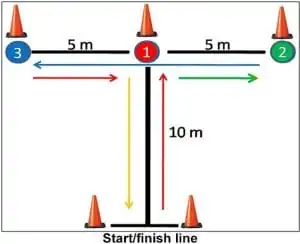
Instructions for an agility T-test: Run 10 meters forward, sidestep five meters right, sidestep 10 meters left, sidestep five meters right, backpedal 10 meters to finish. Do three max-effort, timed trials and take the average of the three.
The authors also concluded that decreased hamstring-to-quadriceps ratio of the involved leg at 60°/s on the isokinetic machine was associated with an increased risk of ACL graft tear. This highlights the importance of hamstring strengthening in an ACL knee injury therapy program.
A physical therapist is trained and can develop a comprehensive rehab program that addresses all the criteria listed above. Many people return to sport or activity without getting enough strength back in their quadriceps. This tends to be highlighted on the isokinetic testing. The bottom line: you shouldn’t leave the health of your knee to chance.
See a physical therapist and get cleared by passing these tests before returning to your favorite sport or activity. If you have questions or are looking for a professional who can develop and implement a knee injury therapy program after ACL surgery, stop by or call our Glendale physical therapy location or one of our many other clinics.
References:
- Joseph, A., Collins C., Henke N., Yard, E., Fields, S., Comstock, D. “A Multisport Epidemiologic Comparison of Anterior Cruciate Ligament Injuries in High School Athletes”. Journal of Athletic Training. 2013;48(6):810-817.
- Paterno, M., Rauh, M., Schmitt, L., Ford, K., Hewett, T. “Incidence of Contralateral and Ipsilateral Anterior Cruciate Ligament (ACL) Injury After Primary ACL Reconstruction and Return to Sport”. Clinical Journal of Sport Med. 2012 March;22(2):116-121.
- Kyritsis, P., Bahr, R., Landreau, P., Miladi, R., Witvrouw, E. “Likelihood of ACL graft rupture: not meeting six clinical discharge criteria before return to sport is associated with a four times greater risk of rupture”. British Journal Sports Medicine. 2016;50:946-951.


